

This piece was first posted on Substack. To comment, please go there.
At core, public health aspires to strike a balance between the moral and the empirical case for health. I have long thought that at times public health arguably did not go far enough in advancing the moral case. This is what motivated me to argue in the past for an epidemiology of consequence. In that, and subsequent writing with Katherine Keyes, I argued for an approach to public health which, at its core—guided by the moral imperative of generating health for the greatest number of people—aims to apply its empirical knowledge to the pursuit of a healthier world. This means prioritizing, on moral and empiric grounds, engagement with the issues that matter most for health, our research guided first and foremost by the demands of human need, with an eye towards doing the most practical good.
In recent years, the pendulum has indeed swung in this direction, towards a consequentialist public health guided by the moral case for health. Our collective balance, our effort to find the right mix of moral and empiric motivation has been tested perhaps like never before during COVID-19. This is understandable. Issues of consequence for health are, by definition, matters of life and death, which concern the wellbeing of everyone—both present and future generations—and matter with particular urgency when we are all, or some of us are, vulnerable. COVID-19 has been particularly troubling as we often found ourselves needing to make a moral case faster than empiric evidence was readily available. And yet, despite this challenge, it continues to seem to me important to make sure that for our arguments to most successfully support health, they should aspire to strike a balance between the moral and the empirical. And that this is perhaps even more the case in a time of crisis. This essay reflects some thoughts on how we can regain, and maintain, this balance.
The below grid is meant to help visualize how we might approach this. It was inspired by Donald Stokes and his book, Pasteur’s Quadrant: Basic Science and Technological Innovation. Each of the grid’s quadrants contains an action which could arguably help create a healthier world. The quadrant at the top left is for steps for which the empirical case is strong, but the moral case needs development. The bottom left is for steps for which both the empirical and moral case need development. The bottom right is for steps for which the moral case is strong, but the empirical case needs development. The top right is for steps for which both the empirical and moral cases are strong—this is where all our arguments should aspire to live.
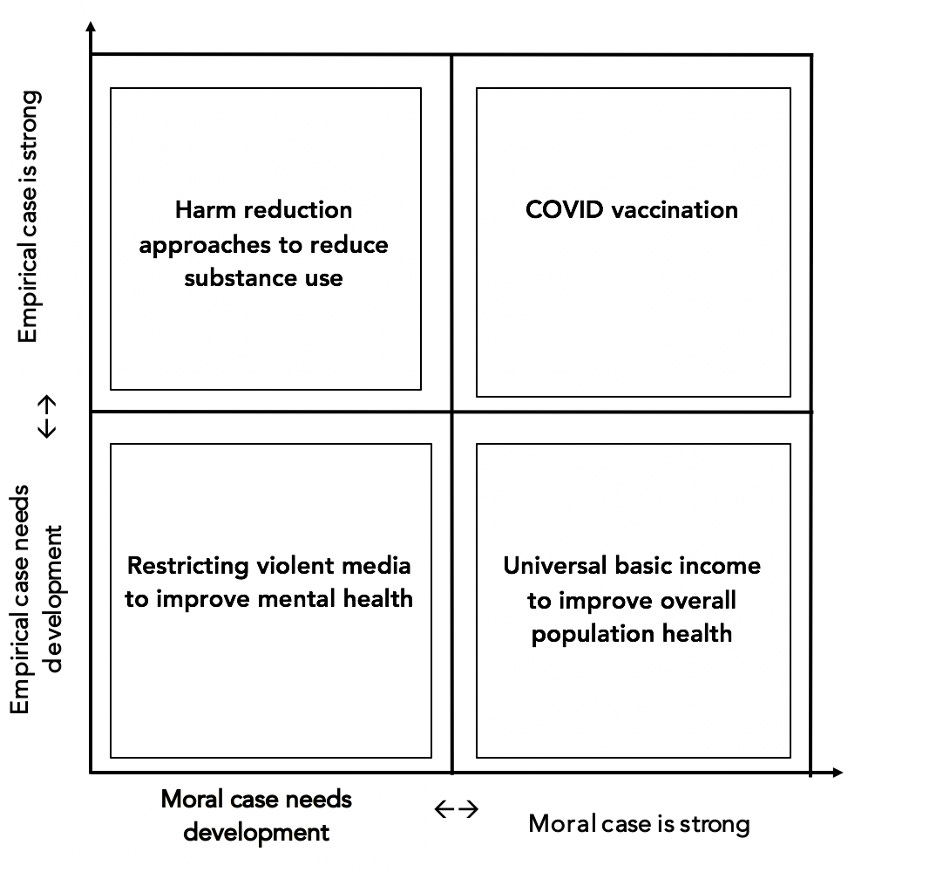
By way of example, I have placed in the top left quadrant harm reduction approaches to reduce substance use, where the empirical case is strong, but the moral case needs development. There is some evidence that these approaches to substance use, such as needle exchanges, can indeed achieve success in reducing harm. Despite these data, the moral case for these approaches is complicated by the impression that they can seem to condone the use of substances, by aiming to mitigate harm rather than by prioritizing a zero-tolerance approach. This places these approaches in a category where they are supported by data but not yet by a fully-articulated moral case that has cleared the way for their widespread use.
Below harm reduction is the case for restricting violent media to improve mental health. This reflects a case where both the empirical and the moral argument need development. At a surface level, the idea of restricting violent media can seem to have merit. We know, for example, that images of trauma can inform the development of depression and PTSD (prior work on this here). Yet, from an empirical perspective, there are not enough data to conclude that banning such media would be an unalloyed good for mental health. Some data suggest, for example, video games—a frequently cited form of, at times, violent media—can be beneficial for wellbeing. At the same time, the moral case for banning such media is complicated by such a ban’s resemblance to censorship. Given the difficult ethical questions surrounding such a step, a potential restriction on violent media occupies the weakest position on the grid, with little by way of moral or empirical support.
In the bottom right quadrant is the case for embracing universal basic income (UBI). This reflects a case where the moral argument is strong, but the empirical case needs development. There is much potential in UBI to help create a healthier country. I have often written about how health depends on being able to access the material resources money buys. It is also the case that many lack access to these resources due to socioeconomic structures which favor people who already have much and disfavor those who have less. For these reasons, it is easy to make the moral case for UBI. Yet, while we do know much about the link between money and health, we do not know much about the link between UBI specifically and health. Because UBI has not yet been enacted on a national scale in the US, we do not yet have data on how it would affect health in the near- and long-term. We can hypothesize, with a fair bit of confidence, that it would significantly improve health, but until we have data we cannot truly know. This means that while the moral case for UBI is strong, we should proceed with due humility about the limits of our current understanding of its enactment on a national scale.
Finally, in the top right quadrant, there is the case for COVID vaccination. Of all the arguments presented on the grid, this one is best-positioned, the moral and empirical case, at this stage of the pandemic, equally strong. The data on vaccine effectiveness are clear, as are the data on the danger of going unvaccinated. Equally clear is the moral importance of getting vaccinated for our own sake and for the sake of our community. The moral case for vaccination, for example, was well-articulated in a recent STAT News article urging the mandated vaccination of healthcare workers, where they wrote:
“Leadership requires taking the moral road even when it isn’t popular. And medical ethics — backed by recent regulatory and court decisions — supports the mandate decision as the best course for the nation’s health.”
While the strength of the case for vaccination has, sadly, not yet been enough to persuade everyone to get the shot, this hesitancy is not for lack of overwhelming support, by both the data and the urgings of basic morality, in favor of vaccination.
It is important to note that, even as we strive for a balance between the moral and empirical case for health, we need not wait until this balance has been achieved before making our arguments. It is often the case that the empirical components of an argument can exist long before a sense of moral urgency reaches a point where it can be fused, in the public debate, with the data that support it. When the US engaged in a renewed conversation about race last summer, for example, it was informed by years of data reflecting the link between racism and poor health. These data were known to us in public health, but they had not yet intersected with the collective moral urgency needed to truly inform the national conversation—until, all of a sudden, they did.
Germane to this, the economist Milton Friedman once said:
“Only a crisis – actual or perceived – produces real change. When that crisis occurs, the actions that are taken depend on the ideas that are lying around. That, I believe, is our basic function: to develop alternatives to existing policies, to keep them alive and available until the politically impossible becomes the politically inevitable.”
I realize it is somewhat ironic to quote Friedman in an essay which aims to help advance progressive reforms of which the libertarian economist might not have approved. Yet his words are, I think, relevant. They speak to the core importance of laying the empirical groundwork for the polices that support health well in advance. We can then elevate these data in the public debate, with an eye towards sparking the moral urgency to match the force of our data. Both the moral and the empirical case are ultimately necessary, if we are to make the strongest possible argument for health. Aspiring to strike this balance should be at the heart of our thinking about how we create a healthier world.